Parkinson’s disease, (PD) is a chronic neurodegenerative disorder. This disorder primarily affects the motor system, but also can impact behavior and sensory systems. In late stages, Parkinson’s can lead to Parkinson’s disease dementia.
Cause of Parkinson’s
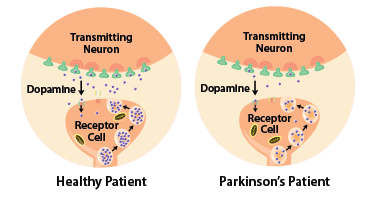
The cause of Parkinson’s is the increase of neuron death in the substantia nigra. The substantia nigra, a part of the midbrain, is responsible for supplying dopamine to the basal ganglia, and is responsible for rewarding movement. Cell death in the substantia nigra is caused by the aggregation (clumping) of the alpha-synuclein protein. Normally, the alpha-synuclein proteins are mostly synthesized in presynaptic terminal (axons). This protein, when aggregated, clumps up into structures inside the neuron called Lewy bodies.
The alpha-synuclein protein is encoded by the SNCA gene. Under normal conditions, the alpha-synuclein protein is soluble. However, mutations in the SNCA gene, among other factors result in insoluble alpha-synuclein proteins.
Parkinson’s is also related to several genetic risk factors. There have been 90 identified genetic risk factors, but the most important one is a mutation in the gene, GBA1. This mutation is found in around 7% of all Parkinson’s cases.
Symptoms
There are two categories of symptoms regarding Parkinson’s disease. One is motor related symptoms, such as tremor slow movement, rigidity, and shuffling, while the other symptoms are non-motor based.
- Motor Symptoms: The most common sign of Parkinson’s is a tremor in the hand. Initially, this only appears in one hand, and when that hand is at rest. However, this can escalate to where the patient is unable to hold anything with their hands as the disease progresses. Another common motor symptom is Bradykinesia. Bradykinesia is the scientific name for slowness of movement. This results in slower walking, and difficulties with feeding, and dressing. Bradykinesia is the symptom of Parkinson’s that most affects a patient. Other motor symptoms are rigidity and postural instability. Initially, rigidity affects the back and neck muscles, and signals the start of increased tremors. As the Parkinson’s worsens, the rigidity can spread even to face muscles. Postural instability comes as a result of the other three motor symptoms of Parkinson’s, leading to a inability to walk, and balance. The instability results in several falls, which also leads to several bone fractures.
- Non-Motor Symptoms: The most common non-motor symptoms are those of cognitive problems. These problems result in a inability to plan, concentrate, and think abstractly. Furthermore, memory, and vision is impacted by Parkinson’s.
Drug Treatments
One major problem caused by Parkinson’s is the lack of dopamine in the basal ganglia. Since dopamine has been found to play a role in invigorating movement, a lack of dopamine negatively impacts movement. Therefore, most Parkinson’s drug treatments focus on providing extra dopamine.
- Levodopa: The most common drug used by Parkinson’s patients, Levodopa is used to provide dopamine to the basal ganglia. Dopamine, as a chemical, is unable to cross the blood-brain barrier, and thus any dopamine supplements taken do not benefit Parkinson’s patients. However, a close relative of dopamine, levodopa, can cross the blood-brain barrier. Once it crosses the barrier, it converts into dopamine, thus providing dopamine to the basal ganglia. However, there are problems with levodopa. Only 5-10% of the ingested levodopa is able to cross the blood-brain barrier. The rest of it converts into dopamine in other parts of the body, causing side effects such as nausea, and orthostatic hypotension (a type of low blood pressure that comes when one stands up). To counter these side effects, patients often take levodopa with carbidopa or benserazide. These two drugs have two important properties: they inhibit the conversion of levodopa into dopamine, and they cannot cross the blood-brain barrier. Thus, to an extent, they prevent levodopa from converting into dopamine outside the brain, thus reducing the side effects.
- COMT Inhibitors: In the blood-brain barrier, Catechol-O-methyltransferase (COMT), is the enzyme that prevents levodopa from crossing. Thus, COMT inhibitors such as opicapone, and entacapone are used with levodopa. Another COMT inhibitor, tolcapone, used to be given as medication, but was found to cause sever liver problems.
- MAO-B Inhibitors: Drugs such as safinamide, selegiline and rasagaline, are used to inhibit the enzyme, Monoamine Oxidase B (MAO-B). This enzyme is responsible for dissolving dopamine. So by inhibiting MAO-B, Parkinson’s patients cna retain higher levels of dopamine, thus alleviating their motor symptoms.

Leave a comment